
Renowned Malawian gynaecologist Dr Chisali Mhango sheds light on abortion law history, misconceptions, fears and law reform process in Malawi. 
Dr Chisali Mhango
Abortion is a very common universal phenomenon. Since the beginning of recorded history women the world over have terminated unwanted pregnancies. The first recorded evidence of an induced abortion is found in an Egyptian Papyrus dated 1550 BC. Of 213 million pregnancies that occur each year worldwide, 40% are unplanned, of these half end in abortion, and half of those abortions are unsafe, that is 22 million, leading to 47,000 deaths from complications that follow.
Abortion has become a topic issue lately in Malawi. The views expressed are shaped by religious ideologies, ethics, culture and human rights. Unfortunately many who speak on this issue stray from the subject matter. Many reveal misconceptions and myths publicly held regarding abortion law reform.
What really is the issue?
The issue is not whether or not abortion is a good or a bad thing. Neither is it about abortion being legalised because abortion is already legal in this country. The issue is that women are dying in increasing numbers, despite the fact that as long ago as 1930, this country enacted a law specifically designed to prevent or eliminate abortion deaths as our moral duty.
A study in 2009 revealed that 67,300 induced abortions occurred in that year, costing the Ministry of Health about 1US$ million annually to manage resulting complications. A repeat study revealed that 141,0444 induced abortions occurred in 2015, largely because women of reproductive age had significantly increased. If the costing remained the same it means that the Ministry of Health was now spending more than 2US$ million dollars of its meager budget on the management of abortion complications alone each year. This costing does not include the cost of losing women in their productive ages. Unsafe abortion, which the World Health Organization refers to as the silent pandemic, is a thus a public health problem in Malawi in as much as it is demanding increased resources to manage its complications.
The history of abortion in the law of Malawi
Criminalisation of abortion was the first course of action all countries in the world had put in place at one time in their history specifically to eliminate deaths from its complications. This prohibition of abortion predates our monotheist religions of Christianity which started in the 1st century AD, and Islam that started in the 6th century AD, and here is the evidence: Graduating medical doctors are required to take the universal ethics oath referred to as the Hippocratic Oath. It is so called because it was authored in 400 BCE by the Greek physician Hippocrates who lived between 460 BCE and 370 BCE. This Oath has been modified over the years to basically “first do no harm” to the patient. Let us however look at the original oath.
Among the things the doctors had to swear in the oath is the following: “I swear by Apollo the physician, and Asclepius, and Hygieia and Panacea and all the gods and goddesses as my witnesses that …… I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan; and similarly I will not give a woman a pessary to cause an abortion……… So long as I maintain this Oath faithfully and without corruption, may it be granted to me to partake of life fully and the practice of my art, gaining the respect of all men for all time. However, should I transgress this Oath and violate it, may the opposite be my fate.” Insertion of a pessary in the birth canal was the only method of abortion in those days as is still common today.
The physicians taking the oath swore to their earthly gods. Apollo was the Greek and Roman deity of music, poetry, art, oracles, archery, plague, medicine, sun, light and knowledge. Asclepius was Apollo’s son and the patron of healing. Asclepius‘ sign was a rod wreathed by a serpent and the medical profession, including the World Health Organization, have since adopted it as a sign of healing. Hygeia is the goddess of health and one of the five daughters of Asclepius, and Panacea, the cure-all, is the sister of Hygeia. The Bible, in Acts 17:28, makes reference to Apollo’s father Zeus who was revered by the pagans as they swore: “In him we live and move and have our being, which makes us his off springs” (Clear Word version). This is another evidence that prohibition of abortion predates the old testament of the Bible.
The message here is clear: even when performed by medical doctors abortion was fatal until relatively lately when asepsis and advanced skills and antibiotics were introduced. These pagan civilisations, more than four centuries before the Christian era, felt that they needed to discourage women from engaging in a practice which was fatal; at least by denying them the procedure in the medical service. They could not stand by and watch women die from unsafe abortion; it was their moral duty to stop deaths of women from abortion complications; morality therefore exists outside our faiths in good measure.
It is interesting that we continue to have connection with Apollo’s Dynasty of pagan gods today. The most effective drug for malaria is Artemisinin, the discoverer of which, Dr Yu Youyou, received a Nobel Prize 2016. The word comes from Artemis, the twin sister of Apollo who was the goddess of the natural environment from whence the Chinese lady scientist found the plant yielding artemisinin.
The poster below, from the godless Soviet Union of around 1925 warned about unsafe abortion this way: “Abortions performed by either trained or self-taught midwives not only maim the woman, 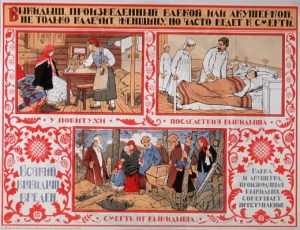
they also often lead to death.” The poster shows a traditional midwife performing an abortion in the top left corner, a doctor doing the same on the right but both women end up in a coffin in the lower part of the poster.
As a British Protectorate, Malawi acquired its abortion laws from Great Britain. Abortion was first codified in legislation in England under sections 1 and 2 of Lord Ellenborough’s Act of 1803. Abortion was then criminalised through the Offences Against the Person Act of 1861. Penalty for procuring abortion then included life imprisonment. Britain proclaimed the British Central Africa a Protectorate in 1889 and ratified it in 1891, renaming it Nyasaland in 1907.
Even after doctors were now able to offer safe abortion women continued to procure back street abortions in England and many of them dying in the process. Abortion, although still criminalized, was then legally permitted in Britain to save a woman’s life through the Infant Life Preservation Act of 1929. Nyasaland adopted the 1929 Britain’s abortion law soon afterwards.
Our legislators were so concerned about saving women’s live that while the punishment for assisting a woman procure abortion or procuring abortion herself in the 1929 law was up to 2 years imprisonment in England, in our country the penalty was raised to up to 7 and 14 years respectively. The procuring of abortion was a crime against the state not God. Here is the reason that Marcus Tullius Cicero, a distinguished Roman politician and lawyer who lived 106 BC –43 BC, gave: “A woman, who inflicts an abortion upon herself deserves the death penalty, as by committing this crime she undermines the power of Rome by depriving it of soldiers.” (Clarae mortes pro patria oppetitae beatae videri solvent)
The current abortion law in Malawi
The law on abortion is governed by the Penal Code Cap. 7:01 of the Laws of Malawi. The current status of the law is that abortion is illegal except where it is performed to save the life of the pregnant woman. This law is modelled on sections 58 and 59 of the England and Wales Offences against the Person Act of 1861 and rules of law relating to the procurement of abortion.
Section 149 of the penal code proscribes the act of assisting the procuring of abortion by whatever means. The offence committed under this section is a felony which attracts a penalty of up to 14 years imprisonment. Section 150 applies to a pregnant woman procuring her own abortion. The offence committed under this section is also a felony attracting a penalty of up to 7 years imprisonment.
The law nonetheless allows the termination of pregnancy where it is necessary to save the life of the mother through Section 243 of the Penal Code. This is modelled on the 1929 of Infant Life Preservation Act which replaced the more strict Act of 1861. Strictly speaking, it also limits this to a surgical operation because at the time it was authored, abortions were only procured through a surgical operation. Most abortions today are procured through the administration of medicines; this alone calls for the revision of the law.
The proposed Bill to replace the current penal code
Proposed grounds for lawful termination of pregnancies suggested by the Special Law Commission on the Review of the Law on Abortion in Malawi are that abortion shall remain illegal but having considered all the information and literature available to the Commission, the exceptions under which abortion shall be permitted should be increased from the single exception to the following four exception:
- where the continued pregnancy will endanger the life of a pregnant woman;
- where the termination is necessary to prevent injury to the physical or mental health of the pregnant woman;
- where there is a severe malformation of the foetus which will affect its viability or compatibility with life; and
- where the pregnancy is as a result of rape, incest or defilement.
Increasing the exceptions aims at increasing the number of women who would qualify for safe abortion, thereby reduce on the number that would resort to unsafe abortion. That should reduce deaths from complications of unsafe abortion. Of interest also is the fact that incest is not a sin in that the eight children of Adam and Eve were to procreate among themselves. It has since transpired that children born out of such relationships have high levels of abnormalities that take a lot of national resources to sustain their lives. Incest is therefore a crime against the state. An interesting case arose in the UK some years back when a middle aged woman had consensual sex with her 18 year old son. When she was taken to court, she produced a document from the Department of Health that reported that women above the age of 40 years, like herself, were not giving birth in that country thereby removing the grounds under which she was being prosecuted.
The case for abortion law reform.
All laws of a country are there for the good of her people. They are not there to punish or harm the people. The abortion law in Malawi was introduced not to protect religious beliefs in our secular country, rather it was to save our women’s lives. Malawi has on many occasions reformed laws that were seen not to serve the people well. Recently the Age of Marriage for girls was raised by reforming the law to better meet the aspirations of Malawi. Currently the country is reforming the 1911 Witchcraft law to be in line with our current interests.
The abortion law in both Malawi as in the United Kingdom from where it originated did not stop women aborting unwanted pregnancies. As to which women were procuring abortion national studies reveal that all social classes and religious affiliations are represented among women seeking care for complications of unsafe abortion as can be seen from the table below.
| Characteristic | Number | Percentage |
| Rural residence | 1375 | 64.4 |
| Education | ||
| No schooling | 257 | 12.1 |
| Junior primary (1-5) | 531 | 25.1 |
| Senior primary (6-8) | 614 | 29.2 |
| Secondary and higher | 645 | 33.6 |
| Religion | ||
| Catholic | 478 | 23.2 |
| Protestant/ Presbyterian | 584 | 28.7 |
| Muslim | 215 | 10.3 |
| Other Christian | 472 | 22.5 |
| Other | 301 | 14.6 |
| No religion | 15 | 0.7 |
Irrespective of their religious affiliations, Catholic, Protestant, or Muslim; despite the fact that almost all of the women had admitted that they knew or had heard of someone who had died from complications of unsafe abortion; and despite the fact that the punishment for procuring abortion is very severe, women were still procuring unsafe abortions when they had unwanted pregnancies; in the process many of them die or suffer severe injury. Here is what women said in the 2009 abortion study in Malawi “When a woman decides that she does not want a pregnancy, she will do anything to terminate that pregnancy”
As soon as evidence revealed that women who terminated their pregnancies under ideal medical conditions did not die the countries from whom we borrowed our abortion laws immediately reformed their laws; after all that was what the restrictive abortion laws were intended to do; eliminate women’s deaths from complications of abortion; it would be a violation of women’s right not to do so. Currently 80% of the world’s population live in countries where safe abortion is legal. The remaining 20% are mostly in developing countries of Africa and South America. It appears to me that the difference between developed and developing countries lies in the fact that in developed countries people mostly think with their brains while in developing countries people prefer to think with their hearts. The debate on abortion in America is just as fierce today as it was when the abortion was legalised in that country in 1972, but there is a gentleman’s agreement that the debate will continue but in the mean time women will not die from complications of unsafe abortion; women will access safe abortion until other more acceptable form of preventing those deaths is secured.
Basis for opposition to abortion law reform in Malawi
Opposition to abortion law reform is based on myths and weak grounds. Weak because if the law is seen not be achieving its intended purpose while the problem of abortion is growing common sense leans on law reform. Myths are numerous; they include the following: a) that abortion law in Malawi is restrictive because Malawians are a God-fearing people; b) abortion law reform is a foreign concept; c) reforming the abortion law raises maternal deaths by fueling HIV as in the Republic of South Africa; d) supporters of abortion do not consider the rights of the unborn baby; e) Nkhoma Mission Hospital has demonstrated that abortion is not a major cause of maternal deaths in Malawi; f) Malawi has no capacity to cope with delivery of safe abortion; g) reforming the abortion law will increase abortion rate in the country; h) family planning can eliminate the abortion problem in Malawi; and i) support for abortion will lead to regime change. I will now try to clarify all these misconceptions with facts on the ground.
The Abortion Law in Malawi is restrictive because Malawians are a God-fearing people.
My jaw drops when people have asked me whether or not I believe in God as I support abortion law reform. This kind of thinking is not unique to Malawi. When I visited Mbabane, Swaziland some years ago I saw a large billboard with the message “THERE IS NO SAFE ABORTION. ALL ABORTIONS LEAD TO HELL” A lot of people all over the world are opposed to abortion law reform on religious grounds because they think that prohibition of abortion stems from our religions and fear of God. Nothing is farther from the truth. As explained above, abortion is a health issue since its inception, before we gentiles knew Yahweh. Abortion is not a religious issue. Those who deny women abortion on religious grounds are actually condemning women to death because they are considered sinners. This reminds me of Saul, the self-confessed chief of sinners, who was confronted on the road to Damascus, and later became the greatest role model for Christians. A religion which says that “because it is the woman’s choice to procure abortion let her die” is a bad religion. A good religion will want to give these women a chance to live, so that they, like Saul, may also have the opportunity to travel on the Damascus road and be saved. Christ knew that if He had just struck Saul dead, the world would have lost a great deal.
Abortion law reform is a foreign concept
The first person I heard say this was a clergy man, although I have since heard the Director for Clinical Services in the Ministry of Health say the same. I know that when white people came here as missionaries they found us worshipping our ancestors’ spirits. When we did not have rain, we brew beer and threw a feast to the spirits and the rain came; so I am told. The foreigners persuaded us to switch to Yahweh instead and we agreed without arguing with them that such idea was a foreign concept. The same white people have come to tell us that the abortion problem we are grappling with, they too had it and they resolved it through law reforms; they share statistical evidence. This time however we are to say this is a foreign concept; likewise the Director of Clinical Services in MOH is championing foreign western medicine instead of promoting our traditional medicine; my mind doesn’t boggle because I know that not all foreign ideas are bad. It is a waste of time and resources, including women’s lives, to reinvent the wheel.
Reforming the abortion law raises maternal deaths by fueling HIV as in Republic of South Africa
I have heard the “Christian Doctors” leadership make this statement and later Reverend Nick Chakwera made the same allegation on Times Television. This is deceitful and therefore unchristian. It is based on the premise that Malawians have forgotten that in this country maternal death ratio rose from 620 per 100,000 livebirths in 1992, to 1120 in 2000 as a result of HIV. This happened under our current restrictive abortion law. What we know is that Malawi could not afford to provide ARVs that time, while South Africa was toying with the idea that HIV did not cause AIDS but poverty. These Christians deliberately suppress the information that since South Africa started to provide safe abortion in 1997 by 2005 unsafe abortion related deaths had been reduced by 91% and the incidence of infection resulting from abortion decreased by 52%. Researchers say that the reason why abortion deaths were not completely eliminated is that while there are 4000 health facilities in South Africa, only 500 of them are registered as safe abortion providers. In other words, access to safe abortion is not up to the desired level.
In the medical field, we use the best medicine we have at any time to treat disease or promote good health. Sometimes, the best we have is also toxic causing fatal harm to some patients. The moment we develop a better drug, we drop the earlier one and use the more effective or less toxic drug. For example, many people in this country died as soon as they initiated the earlier antiretrovirals. We nonetheless used them because many other people benefitted from them. We have since developed better drugs and we have abandoned the less acceptable medicines. We no longer beat mad people into submission, we use drugs to calm them. If a doctor says that because of his faith he will not use the toxic medicine that will perhaps save the mother but in the process kill the unborn baby, that doctor is dangerous and not fit to practice medicine by the standards of all medical councils in the world. Obviously, the moment we shall develop a process which will eliminate the abortion deaths without resorting to provision of abortion, I will be the first to switch to that new approach.
As to whether liberalising the abortion law can reduce maternal deaths, Romania is classic example as documented by Serbanescu’s team in 1995. Abortion by skilled medical personnel was legally available in Romania in 1957. As can be seen in the graph, abortion deaths (shown in yellow) plus deaths from childbirth (shown in green) equals total maternal deaths shown in red. The total maternal deaths were relatively low and falling at that time. In 1966 the government of President Nicolai Ceausescu, a devout catholic, reversed the abortion law through a Decree. The result was a sudden and sharp escalation of total maternal deaths, mostly due to unsafe abortions as deaths from childbirth continued to decline as can be seen in the graph. When a popular revolt had President Nicolai Ceausescu assassinated and safe abortion made legal again, maternal deaths plummeted. Worldwide studies reveal that where abortion is legal and permitted on broad grounds, deaths from complications of unsafe abortion are rare, but where it is illegal abortion is often fatal.
The demonstration by the clergy also is surprising because the three groups that organized the march were all represented on the Special Law Commission that has come up with the proposed Termination of Pregnancy Bill. The Draft Bill presented to government has signatures of a Senior Catholic priest, a Bishop representing the Malawi Council of Churches, and a lawyer representing the Muslim Association of Malawi. These were sent to the Commission by their institutions. What do the clergy expect the parliamentarians to make of those signatures I wonder.
Supporters of abortion do not consider the rights of the unborn baby
The current abortion law permits abortion when the life of the pregnant woman is threatened in such a way that she could die if the pregnancy continued. A legitimate concern has therefore been raised by some that while the pregnant woman is granted her right to life, a similar right to life has been denied for the unborn “child”. The response to this ethical concern is that studies from Malawi and all other countries is that denying a woman safe abortion does not make her keep the pregnancy. If it did there will be no abortion deaths and the abortion problem would not exist. What actually happens is that denying women safe abortion just pushes them to the unsafe abortion option. This means that we do not save the unborn babies but in the process we lose many mothers also. Here is a true story of the case of a couple who visited one of our hospitals to seek abortion. The woman was screened and found that she did not qualify for abortion on the current law. A week later the husband brought the wife in critical condition after unsafe abortion. She died a few days later leaving behind three young children, including a toddler. Studies all over the world reveal that most toddlers whose mothers died also died. This case illustrates that doctors, even with the involvement of psychiatrists, are not always able to detect threat to the woman’s life if the pregnancy continued and therefore sometimes they deny women abortion even when they were legally entitled to it under the current law.
Secondly it is noted that before abortion was codified in the English law, abortion was dealt with under the Catholic Ecclesiastical courts. In these courts, if a woman procured an abortion after “quickening”, when the fetus was considered to have gained a soul, the punishment was death. Before this period of pregnancy the punishment was something like forty days penance, not death. It is clear that, as George Orwell has told us in book Animal Farm, while all animals are equal, some are more equal than others. I believe that the reason why the Special Law Commission has recommended that a woman who seeks abortion after being violated through rape, should do so only before the pregnancy has passes 16 weeks of age. This is not biblical; it comes from Aristotle, a Greek philosopher and scientist (384 -322BC), who taught that the human soul entered the forming body at 40 days in the male fetus or 90 days in the female fetus, and quickening was an indication of the presence of a soul.
I take it that His Grace, Archbishop Thomas Msusa, agreed with this thinking when he was quoted in the Nation of 11th November, 2016 as saying “If we accept the change of the law on abortion then the future of this country will be bleak, …. The next generation depends on us taking (care of) the children and the unborn.” It means that His Grace accepts the current law which puts the life of the pregnant woman whose life is threatened above that of her unborn child because he did not call for the scraping of the current law.
Thirdly, if I kill somebody for whatever reason, and the people around start lynching me, the police will snatch me to safety. In so doing the police are not saying that what I had done was good and acceptable. What the police have always said is that the country having lost one person should not lose another; the guilty party will still have his day in court and bear the consequences or with his maker later. And so it is with abortion; you either lose only the baby by granting the woman safe abortion or you lose both the baby and the woman by pushing her to unsafe abortion.
It has been said that every country has a Maternal Mortality Ratio its Government deserves. Most maternal deaths are preventable and solutions to eliminate them are known. What is needed is commitment to put in place not only the requisite resources but also the appropriate legal environment to address the causative problems. Some have said that the reason why 18% of maternal deaths in Malawi are due to abortion is because of high case fatality rates in our hospitals. At Nkhoma Mission hospital only 6% of the maternal deaths were due to abortion. This is an erroneous thought process. The top five causes of maternal deaths in Malawi are haemorrhage (24%), which is mostly bleeding after childbirth; sepsis (24%), which is mostly infection after childbirth; obstructed labour (20%), mostly in young women as a result of being pregnant before their bony birth canals have grown to full size; complications of unsafe abortion (18%); sudden rises of blood pressure during pregnancy or childbirth (12%); and other causes (2%). If 18% of the maternal deaths in Malawi are due to unsafe abortion, it means 82% are due to the other causes. If at Nkhoma hospital only 6% of the maternal deaths are due to abortion, it means 94% are due to other causes. Where is the wisdom of considering 94% to be better than 82%? In England, the abortion law was reformed in 1967 when abortion deaths contributed 14% of all maternal deaths; similar to our 18%.
Firstly unless a woman is stranded she will not seek care for complications of unsafe abortion from a hospital owned by a people who stigmatize abortion. Nkhoma hospital does not receive the same number of abortion cases as government institutions which contribute more representative statistics for Malawi. Secondly poor women do not seek their services from fee paying institutions like Nkhoma hospital. Deaths from complications of unsafe abortion are a problem of poor women. In our study this is what women in rural areas said “This problem is with the poor, because they seek their (abortion) services from traditional healers and it is only known when they have complications. It is all about poverty; the rich are sorted out with their money”.
One effect of reforming the law and thereby make safe abortion available in public hospitals will be to bring equity in health care between the poor and the non-poor. Facts on the ground are that abortion on demand is quasi-legal in Malawi in that many women in urban areas admit to procuring abortion when they so wished from various fee paying sources. The problem is that poor rural women in this country are crying foul in that they think the law discriminates against them when they say this regarding availability of abortion services to them: “If you are poor, your voice is nothing. Pregnancy is a death sentence to the poor people.” The objective of Safe Motherhood is to eliminate abortion related deaths. Six percent is not an acceptable proportion of abortion deaths anywhere.
Malawi has no capacity to cope with delivery of safe abortion
This is false because it premised on the thought that if abortion law is reformed, floods of women will present themselves for abortion services. It has never happened anywhere and there is no reason to suggest that Malawi will be different. What happens is that the number of abortions remains the same; law reform simply shifts unsafe abortion to safe abortion.
When safe abortion is permitted, it simply shifts unsafe abortions to the safe abortion option, the total number of abortions remain the same. What this means is that instead of treating complications of unsafe abortions, Malawi would now just be offering safe abortion services. This is a much cheaper and quicker day-care service, as opposed to treating complications of unsafe abortions which requires the services of the hospital for longer period, more complicated treatment including operations to remove rotten wombs, blood transfusion supply and full courses of antibiotics. If we are currently coping with the management of complications unsafe abortion, because we have no option but cope with the situation, how can we fail to cope with the simpler and cheaper process of providing safe abortion?
Reforming the abortion law will increase abortion rate in Malawi
Experience from all other countries have shown that over time abortion rates fall after the abortion law has been reformed. When I worked for the United States’ Centre for Disease Control in Atlanta, operating from the Abortion Surveillance Branch in the early 1980s, the Guttmacher Institute reported that there were 2 million abortions procured each year when the population of USA was about 200 million people. Now that there are more than 300 million people, reports are that there are about one million abortions not the expected 3 million. There is no reason to suggest that this will not happen in Malawi because an abortion service always goes with a stronger family planning component. South Africa, which has the most liberal abortion law in the world, has the lowest abortion rate in our region.
Family planning can eliminate the abortion problem in Malawi.
This argument is promoted by the clergy and it is understandable but ironic. When botanist Marie Stopes opened the first family planning clinic on Holloway Road in London, in 1924, family planning was a dirty word. Surprised by the response, women attending the clinic were asked as to how they had come to know about the clinic. They responded that they had heard it from the church; the clergy told them that a family planning clinic had opened on Holloway Road and they were counselled not to go there as use of contraceptives was considered indecent and sinful. But then religion is dynamic; it is no longer an indecent thing to plan one’s family.
In Malawi however family planning remained a dirty word and an indecent thing to do until relatively lately. We were the last country in the region to adopt family planning. Since then however we have run fast, thanks to USAID and others. We have surpassed countries that started much earlier, including Uganda that started family planning in 1956. Our studies have revealed that the abortion rate in Malawi varies widely by region. The abortion rate was highest in the Northern region (61) and lowest in the Central region (29). These two regions had the lowest and the highest levels of contraceptive use of 54% and 63% respectively, according to the Malawi Demographic and Health Survey of 2015/2016. The Northern region had as a result the highest unintended pregnancy rate and Central region had the lowest. More than half of the pregnancies after the 4th child are unwanted according to the Malawi Demographic and Health Survey of 2010 thereby increasing the abortion option among this group. Expanding access to contraceptives will reduce unwanted pregnancies and thereby reduce abortion rates.
This begs the question, why is it that in the UK and USA where all women have access to family planning these countries still need liberal abortion laws. The answer is found in a USA study of 2008. About 54% of women who had abortion induced in that year had used a family planning method in the months they conceived; the corresponding figure for Malawi in 2009 was 23%. In addition wanted pregnancy can later become unwanted, for example when the putative man aborts or when the once in a life time opportunity for a scholarship turns up. These are the facts of life.
As the graph below shows, we are reaching more and more women with contraceptive services but abortion will continue to occur unless we adopt a strategy that has been shown to work such as abortion law reform. While the Catholic Church is against law reform in Malawi, the church is paying lip service to Natural Family Planning, a very strong arm of the successful family planning programme in Mauritius.
Support for abortion will lead to loss of parliamentary seats at the next elections.
This has been voiced by a number of parliamentarians and it is pure greed of putting personal interest to women’s lives. I repeatedly had argument with Bishop Milingo when I was arguing for the reforming of the abortion law in Zambia where I worked for a long time. Among the threats to parliamentarians was that people will not vote them in at the next election if they supported the Bill to reform the law.
When the Bill went to parliament it was passed. The UNIP government was retained to power at the next elections. What option do parliamentarians have other than take another look at the law and make it effective considering that the problem it was designed to resolve was growing. Abortion law reform is not about the rights and wrongs of termination of pregnancy. Law reform is justified only if there is evidence that there is need to do so. The fact is that the Penal Code on abortion in Malawi has not prevented women from dying from complications of unsafe abortion as has been the experience of the country that gave us this law. There is need to replace it with an effective law as other countries that have had this law have done.
When politicians in Canada could not agree on the abortion legislation, they just agreed that this was a medical problem and left it to the Ministry of Health to deal with. There is no legislation for doctor to perform Caesarean section, for example, why did they have to register for this other medical problem? In Canada women have access abortion freely as a normal medical service. There is today increasing debate in the UK that the country should follow the Canada example.
Some have expressed fears of abuse of the law when it is liberalised. While working in England, twice a lady with an Irish accent, called me from the Department of Health to seek clarification as to why I have performed certain abortions. She on both occasions accepted my reasons. The message is that the Ministry of Health will always put in place mechanisms to monitor possible abuse including quality of care.
Gynaecologists are biased on abortion law reform
A statement has also been made to the effect that we members of the Association of Obstetricians and Gynaecologists of Malawi are biased in our presentation of the abortion problem in Malawi. The fact is that we have been admonished by Professor Türmen, Executive Director at the World Health Organization who said in 2000: “It is not enough to be clinically competent. It is not enough to be socially aware and socially conscious. The obstetrician and gynaecologist must be a champion for all women’s health, welfare and rights… their leadership and their social and economic clout are needed to make essential obstetric care available to all women.” When a woman dies during pregnancy, it is considered the fault of the Obstetrician. It is therefore the responsibility of obstetricians to advocate for the removal of obstacles in the system, such as reasons why blood was not available to the bleeding woman, why essential drugs were not available for the woman with fits, and why appropriate legal environment to prevent the pregnancy related deaths was not in place.
Professor Mahmoud Fathalla, also Director at WHO and founder of the Safe Motherhood Initiative once said and we agree “—-women are not dying because of diseases we cannot treat. They are dying because societies have yet to decide that their lives are worth saving.” Ann Firth Murry, founding president of the Global Fund for Women, adds: “The promotion of women’s health and especially their Reproductive Health is not just a good, political, economic or development decision; —- it is the right thing to do”
Dr Chisali Mhango, Fellow of the Royal College of Obstetricians and Gynaecologists, is Honorary Senior Lecturer at the College of Medicine of the University of Malawi and visiting Obstetrician and Gynaecologist at Mwaiwathu Private Hospital. E-mail: cmhango@globemw.net